On Friday 4 April, the final seminar for MedTechLab's course in ‘Acute stroke, diagnosis and treatment’ was held at BioClinicum in Solna. 16 course participants received a full-day summary and discussion on the diagnosis and treatment of stroke and cerebral ischemia.
The seminar was led by Håkan Almqvist, Consultant Neuroradiologist, CAPIO S:T GÖRANS SJUKHUS AB (right), Åsa Kuntze Söderqvist, Consultant, PhD, Neuroradiologist and Neurointerventionist. ME Neuroradiology, Karolinska University Hospital (middle), and Michael Mazya, Consultant, Associate Professor, Neurologist. ME Neurology, Karolinska University Hospital (left).
“I think it was a successful course. We had participants from many parts of the country and had a good discussion where many were active. The fact that the course participants are radiologists, neurologists and internal medicine specialists favours the discussions and increases the understanding between participants with different specialties about how they think and make decisions about treatment,” said Åsa Kuntze Söderqvist afterwards.
Håkan Almqvist said that part of the discussion was about how the investigation is organised in different regions affects how an acute stroke investigation is carried out. Some regions have purchased automatic interpretation of CT perfusion, but not Region Stockholm, for example, where the distances are shorter, and the triage of patients is slightly different. However, Karolinska has extensive experience of CT perfusion, which has been used for about 20 years in connection with acute stroke investigations.
“The future AI support in stroke investigations may be based on a CT/MR perfusion to find even more peripheral vascular occlusions, provided that endovascular reperfusion has a positive effect. This course provides the basics of what perfusion disorders in the anterior circulation look like and there are some pitfalls. There are some difficulties in stroke investigations, especially in the posterior circulation where perfusion software works poorly today. Therefore, it is good if many have attended courses dealing with acute stroke”.
A new round of courses will be held in autumn of 2025.
Since 2023, MedTechLabs organises a hybrid course in acute stroke, diagnosis, and treatment. The course is Lipus-certified and is aimed at residents and specialists who are interested in learning more about stroke and cerebral ischemia. One of them is Kristoffer Linder, a specialist in neurology at Capio S:t Görans Hospital, in Stockholm.
Hi Kristoffer, why did you choose to take our course?
I thought it sounded like an interesting approach, it was not like any course I had taken before. I got a tip about it via an email from a colleague. I thought that when you work in an acute hospital that receives a lot of acute stroke cases, it might be valuable to attend. In the hospital where I work, we take care of almost 1,000 patients with stroke or TIA every year. I also saw that there were many interesting names as lecturers as well, such as Håkan Almqvist, Åsa Kunze and Mikael Mazya. Trusted and knowledgeable course leaders give high credibility.
What do you think about the course organisation?
I think they have chosen a good division and balance between the radiology and the clinical parts of the stroke panorama, including a review of trobectomy. For me, it was good and important that you can take the course at your own pace. You watch the videos when you have time and can pause and go back through the material as needed. Otherwise, it can be difficult to get through longer course sections when you are busy at work.
What has the course given you?
The part where you had X-rays available and the opportunity to look at them yourself was very valuable to me. You can’t get that any other way. Of course, there are many databases and websites with X-rays, but here you could scroll through the material and at the same time get the necessary information about the symptoms, how long it’s been since the illness and so on. I have been a specialist for two years and have been working with stroke patients since I became a doctor more than ten years ago, but it was very good to be able to get this refresher course. The investigation and treatment of stroke has changed a lot in recent years but it’s also good to go back to basics, which this course also addresses.
Who do you think should take the course and why?
Can I answer everyone? Primarily those who are in training or already working as doctors. Both residents and specialists who have been working for a while can benefit greatly from the course. The course is good for updating your knowledge. I think it is also valuable for medical and radiologists working with stroke cases.
In Sweden, more than 18,000 people suffer an acute ischaemic stroke every year. With correct and rapid treatment of stroke, both lives are saved, and the affected person can avoid lifelong disability, something that both provides increased quality of life for the patient and saves big money for society. The new treatment options that have emerged over the past decade require more knowledge in healthcare, which is one reason for the new course offered through MedTechLabs.
The course “Acute stroke, diagnostics and treatment” organised by MedTechLabs started in October 2023. The course is aimed at residents and specialists who want to train in this area to better follow the national recommendations and guidelines for examination and treatment of stroke and TIA. The new course was offered to doctors in Region Stockholm as well as in other parts of the country and was quickly oversubscribed.
We spoke with Håkan Almqvist, senior physician and neuroradiologist at Capio St Göran, who is responsible for the course. Håkan has worked almost all his professional life with stroke, first at SÖS and later as a neuroradiologist at Karolinska and has followed the modern development of how to find and eliminate thrombi/embolisms since the late 90s.
Hi Håkan, can you tell us a bit about the course and why it is given?
“The course aims to provide knowledge about the benefits of acute reperfusion therapy within 24 hours in several patient groups, including those with relatively large established infarcts. The management and assessment of TIA is also included in the course. “The biggest problem with stroke care is still that patients come in too late, so it’s important that everyone in the community knows that help is available and picks up the phone if they have symptoms. But we in the healthcare chain also need to be on our toes and know what is needed for the patients. We must dare to be rational and inclusive, even if there is a low probability of stroke. Because it can be difficult to know whether your judgement is correct. Doctors need to see many cases to become skilled in their judgement and that takes time, especially in a smaller hospital.”
How do you deliver the course?
“In the first round, we offer it free of charge to 40 participants who receive around 30 video lectures and case study material with commentary, which we distribute using Collective Minds Radiology and their radiological imaging system. It is up to the student how much time they spend on that part, but I would say it is about two and a half days, at their own pace. In addition to this, we have a mandatory physical meeting in the form of a seminar in Stockholm where case studies are discussed. The knowledge check takes place at this seminar and active participation is required to obtain the course certificate.”
Who came up with the idea for this course?
“Many of us realised early on that there was a lack of continuing education for the new forms of examination and treatment that have emerged in the field. When MedTechLabs started, it was realised that there was a need for training in the region. Professor Staffan Holmin, together with KTH professor Mats Danielsson, saw an opportunity for the centre to contribute to and provide training. “As early as 2018, we started recording parts of the material that is now used in the course, along with new material in 2023. The pandemic and questions about which platform to use have meant that it has taken some time.”
What do you think has made the course so popular?
“The course only corresponds to a few days where you choose when for about 1 month. That certainly has an impact. But it is up to the student how much time they spend. I think long courses are becoming more difficult to attract. That we have a hybrid approach with self-study with lectures and being able to browse cases combined with a physical seminar with the teachers. A course must also be able to provide both a course certificate and an ST certificate. This is probably exactly what many doctors are looking for in terms of continuing education.”
When will you hold the course next time?
“This is the first time we have held it, and we will of course further develop it based on the feedback we receive from the course participants. Then we will see how many times a year is reasonable. It is also a question for Region Stockholm, which this time allowed doctors from other regions to attend free of charge. But hopefully we will also organise the course in 2024.”
SVT – the Swedish national broadcasting company – highlights the impact of research on AI for breast cancer detection in mammography, conducted by MedTechlabs researchers Kevin Smith and Fredrik Strand. Also, Lancet published a scientific article on the study conducted at Capio Sankt Göran Hospital in Stockholm.

What differences in cancer detection and unnecessary recalls are the results of various combinations of AI and radiologists? Lancet Digital Health has published the results of a prospective clinical trial conducted in Stockholm.
MedTechLabs researcher Fredrik Strand is surprised at how accurate the AI was and says that the potential for AI to handle most of the screen-reading is huge.
Karin Dembrower is chief physician and medical director of the Mammography Department at Capio S:t Göran’s Hospital where the clinical study was conducted. She is very satisfied with the results.
– We found slightly more cancer and recalled fewer women who turned out to be healthy, so we made fewer women worried. And we freed up time for the radiologists to do other diagnostics than looking at mostly healthy women’s images. We have managed to cut the queues considerably so we are a queue-free breast centre now, she says in the feature.
The AI-assisted breast cancer detection system has been operational since summer 2023 at St Göran’s Hospital in Stockholm.
– We have shown that our AI technology works on St Göran and their equipment. But that doesn’t mean that any AI will work on all equipment, so it’s something you need to check before introducing it, says Fredrik Strand in the same feature.
Watch the tv-feature here (in Swedish)
Read the Article in Lancet Digital Health here (full text)
On 19 April 2023, MedTechLabs organised a seminar focusing on strategies for researchers to better identify and protect their digital innovations. Also on the agenda were tactics and practical tips on patenting or other ways to extract business opportunities from science linked to digital applications.
Niclas Roxhed, director of MedTechLabs, began by giving a background to MedTechLabs and its focus on interdisciplinary, translative research in later phases, proximity to clinical trials and clinical implementation, and industrial collaboration. He then gave the floor to Måns Marklund, IP strategist and founder of Cascelotte.
Måns then explained how he and his company have analysed results from researchers linked to MedTechLabs, examined the volume of patents and also made an in-depth study of their quality, potential economic value and technical standard. Compared to some of the world’s best research centres, these patents were found to be of a very high standard, especially those linked to Mats Danielsson and his research teams.
– Other research at MedTechLabs turned out to be more linked to digital applications and artificial intelligence, which may be one reason why this kind of research does not lead to as many patents. After discussions with Johan Schuber, Executive Director of MedTechLabs, we therefore decided to investigate this phenomenon more closely, said Mats.
How good is Sweden in international comparison?
Mats explained the importance of looking at the differences between different kinds of technologies. Normally, Sweden ranks 12th in the world in terms of all technology patents. However, many come from Ericsson, which inflates the volume. In life science alone, Sweden is ranked 15th, which is still very high, and an indication of how good Sweden is even without Ericsson.

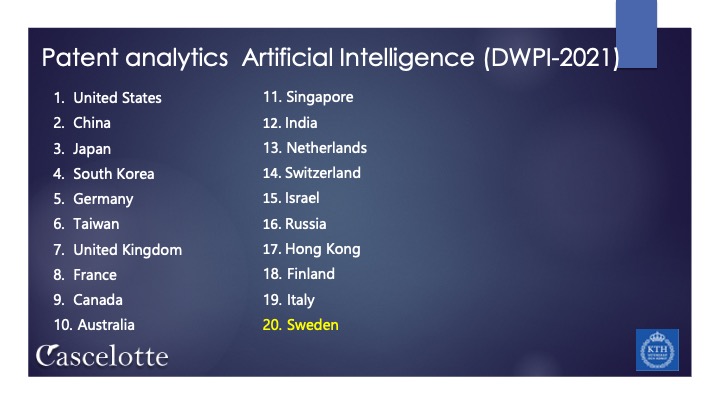
– In AI, Sweden is ranked 20th in terms of patents, also very high considering we are a small country. But perhaps there is room for more patents, with increased knowledge of how this works and why patents should be granted in this area as well. We also know that if there are patents in an area, there are many other intangible assets there. It could be trademarks, knowledge of data and data use, design and so on. So, the patents indicate a country’s ability to transform innovation into economic value, Mats explained.
He went on to add that AI is also one of the most patented assets now, so it is not true that AI cannot be patented, even if it is slightly different from other technologies. This also applies to the life science area in general, compared to other patent areas.
– It is important to understand which strategies, tactics and practical approaches are good to know when it comes to both AI and life science. Therefore, we chose to invite Michael Kitzler and Malin Keijser Bergöö, who both work as lawyers specialised in European patent issues at Rouse, said Mats and handed over to these speakers.
Positions of control and the commercialisation of innovation
– In a commercial context there are some fundamental questions you need to ask yourself, like what you’re selling – sometimes it seems like you’re offering one thing when it’s actually something else. In the context we are talking about now, many of you are probably in an early phase of commercialisation, maybe you have created a company and you have something to sell to someone, Michael began.
He then described how Rouse usually starts by identifying the intellectual assets that the research team or company has built up over time and then translates these into different “control positions”, which he explained as the aspect of control that creates ownership and/or control over an innovation over time. Some of these can be patented, some may need to be kept secret until later, some can be contracted with other actors, and some are based on a unique combination of capabilities that are difficult for others to acquire.
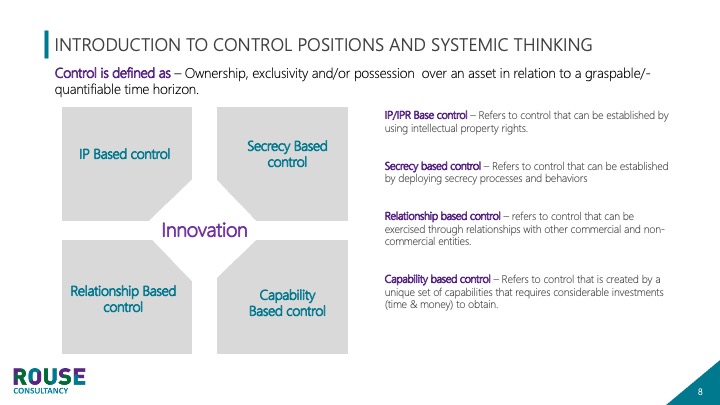
He explained that different companies/teams need different mixes of control over assets and gave the example of a company that had 55 per cent of its assets covered by patents, 25 per cent by external agreements of some kind and 10 per cent by secrecy-based control. Software and IT companies tend to have fewer patents and are more likely to use other methods, while high-tech companies put a lot of effort into getting patents. Michael argues that medtech companies are somewhere between high-tech companies and software companies in terms of control positions.
– Looking at the trends in medtech, the statistics show that there are more patent applications in this industry than in others. So, is it worth the money to make these applications? Probably, said Michael.
The largest patent owners in medtech include companies like Siemens Healthcare, Philips, Fujufilm, Canon Medical Systems and Merative. Then there is a “long tail” of companies that may not have as many patents, but these can be very important. Michael gave the example of Elekta, with only 12 patents in the field of AI, but which are very significant. Even further down the list, there are companies with maybe four patents, which can be very relevant portfolios despite their small number. To summarise, it doesn’t take many patents to make a difference and achieve commercial success, it’s all about the content of those patents, Michael explained.
Michael then listed the commercial values that patent control positions create for medtech companies, from limiting business risks to contributing to the company’s participation in key ecosystems (see image below).
Patenting medtech and AI in practice
– Your field is one of the toughest to patent. Partly because it has to do with things you do with the help of computers, which the patent authorities are very careful about before approving, which makes it complicated and requires more work and the right strategies, Malin began.
She explained that in some countries there is a ban on patenting treatments, which can affect companies, and that you are then allowed to patent the devices you use, not the methods. This differs depending on where you are in the world; in China, for example, it is easier to patent treatments. In Europe, on the other hand, it is often impossible to patent treatment methods. In the US it is more unpredictable, where a single court decision can change the situation so that it suddenly becomes possible to patent something that was previously impossible, and vice versa. Malin emphasised that having said that, it is still often possible to patent – in some way. You may have to go through the equipment instead of the method, or do it in other ways, but it is always possible to patent something.
– One thing we saw when we looked at medtechlabs was projects in bioelectronic medicine where inflammation is reduced by electrical stimulation via an implant. If you want to patent at an early stage here, the concept constitutes a treatment method, which means that you might choose to patent the implant instead. But competing companies may then choose to use a different implant. So very broad concepts can be difficult to patent with commercial success, Malin explained.
She then gave an example of pacemakers. A pacemaker stimulates the heart and is therefore considered a treatment, which cannot be patented in Europe. But the actual method of identifying which signals the pacemaker should use to stimulate the individual patient’s heart in the right way can be patented – if you state that you store this data somewhere and do not use it directly to stimulate the heart. Then, of course, you can also use this stored data to stimulate the heart. An example of how you can adapt the design of patents to the legislation and get an effective patent that provides indirect protection for the treatment method anyway.
Malin also gave the example of a company that has patented a detailed description of how they trained their medical image recognition algorithm, thereby gaining intellectual property protection for their innovation. This protection has been granted worldwide, including in Europe. Another example involved wristbands used to alert an elderly person to a fall. The company used AI and machine learning to correctly interpret the signal from the bracelet. The solution to obtain patent protection here was to focus on specific parameters that were used when the algorithm analysed the signal to distinguish between an accident and the wearer just lying down. Such parameters could be, for example, which room the wearer was in, whether the wearer had moved, slept recently, run, etc. The combination of parameters provided a basis for the way the algorithm works, and this was the basis of the patent application.
– One challenge when you want to patent AI solutions is that you can’t always describe why the solution gives the answers it does, because they are based on an algorithm that has trained itself to find the answers on huge amounts of data, but in patent applications you have to be able to describe this, said Malin.
Michael summarised the need to contextualise AI and gave some key takeaways: patenting can be a powerful tool to control the value-creating phenomena that arise in digital medical technology. However, a systematic approach is required by those who want to create control through patents and other control measures. Finally, patenting in digital medtech is more complex than in most other fields and therefore requires well thought-out strategies. To achieve powerful patents in medtech, you must do the right thing, which often requires a more systemic approach. You also need to understand the full range of assets you have and how they can be used and controlled, concluded Michael.
Questions from the audience
Niclas then moderated questions from the audience, to which the participants provided answers.
Question: What is required to be able to patent an AI model for radiological images?
Answer: The way to build and train the model, e.g. based on specific parameters, if these are very different from other models, then it is easier to patent it, provided it is new. Just using a general model trained on many images is more difficult.
Question: What happens if a researcher has published an academic paper describing such a method?
Answer: It depends on how long ago it was published. In the US, you have one year to apply for a patent after publication without blocking yourself from patenting. In Europe, you must apply before publication. It should be added that academic papers do not always disclose the whole innovation, they can be more general and do not necessarily describe details that make patenting impossible, in Europe.
Q: What happens if you have patented and published something and then want to patent something that is slightly different from what was first patented?
Answer: It always gets complicated if you change things in a follow-up patent application. It is better to have everything worked out and right from the start. But the reality and needs of publishing an innovation may take priority and you should generally file an early patent application; it is better than not claiming your innovation at all.
Q: What does protection mean in practice if a large company infringes?
Answer: Unfortunately, those with the most money win. But if you have a patent, you can enlist the help of another big company to help you win against the infringer. The patent can also act as a deterrent to large companies who don’t want to get into trouble. Large companies may also appreciate that a smaller player talking to them has a patent for their innovation, so that it is clear what it is about.
Question: You can’t patent data, but can you patent the way you curate data when training an AI?
Answer: It depends on whether the approach is very different from how the same thing has been done before. If it is done in a different way, it can work, compare with the example of the bracelet that would warn of falls, where the choice of parameters was part of the curation. Then there is the actual database protection, that you own this data. And when you process the data, a new data set is created, much like the translation of a literary work from Swedish to English. In some cases, it can be difficult to prove who originally owned the data. The EU also requires that certain health data must be made available to other users, known as data sharing.
Q: Does a patent application need to have proof that the innovation works?
Answer: No, normally not. A classic example is the patent protection of perpetual motion machines.
Question: Can recommendations for treatment be patented?
Answer: Yes, the example of the pacemaker is such a case, where the signal to be used for the treatment was first stored and then used.
Question: Is it common for sufficient preparatory work to be done on IP at the pre-commercial stage? Answer: Yes, I would say so (Michael). But you should always make a business case before applying for a patent, because it can cost around one million to do all the IP work, and then you need to know that you will earn at least that amount to make it worthwhile (Malin).
KTH Innovation: we can help in these phases too, for the researchers who need it.
Nicklas: And KI Innovation can also contribute in a similar way.
Niclas: and to present a credible business case, you need to try in the IP area beforehand. This is at least my experience from this area.
Michael: And we’ve said here today that all patents can ultimately be broken by big players, but if you don’t have a patent right from the start, you have no control over what you’ve come up with and no negotiating position.
Niclas: What belongs to the field of medtech is also the long lead times, not least when the innovation is to be tested clinically and then implemented, generating the need for a lot of additions to the patent application.
Question: What are the three most important things to consider for a research group that has developed an innovation and wants to commercialise it in the future?
Niclas: To patent at all. I always suggest it to my postdocs – for every paper, the legal requirement that it is an innovation is there. There should be potential there. For every paper we publish, we submit a patent application, in principle. You also have to consider whether you can get your money back on such an investment. If you don’t see that possibility within a year, you might drop the application.
Question: We talked earlier about how you can’t protect a biomarker, but you can protect technical equipment. Nor can you patent a single molecule, but is it possible to patent a combination of molecules?
Malin: It depends on the country. In the US, you used to be able to patent treatments using a combination of biomarkers, but that is no longer possible. Nowadays this is considered a natural phenomenon that cannot be protected.
Question: how to protect AI innovation in early collaborations between researchers and companies. How do you protect the agreements you make there, when you may not even have published anything?
Michael: This is an important phase where you need to define the origin of the innovation through agreements. Even if it is too early to apply for the patent, the agreement is valid in court. Unfortunately, research teams often settle for agreements that are too general and do not go into the details of who owns what and how this will be handled at a later stage. Again, researchers need to get proper help from lawyers who know this area, because creating these agreements is complicated. I have seen so many cases where it has gone wrong.
Question: How broad can patents for diagnosis based on AI be?
Answer: It depends on whether you put in things like what parameters you used. Just using general descriptions that you used AI is not enough. Then your patent may only cover, say, 17% of the solution you developed. But then you still have protection for that part of the window. Many patents are quite narrow, but if you have the smartest solution, the market will probably not settle for an inferior solution just because it is not protected. And then you have something to sell.